The decision to accept or reject these new terms and conditions is not only about the contract itself, but the context it sits in. In a two-part behemoth blog post juniordoctorblog looks first at the contract, and then the wider situation in the NHS.
Part 1: Let’s look at the contract. Read Part 2 here.
Unsafe?
There has been some movement between the March offer and the May offer on the safeguards for doctors working. The hours limits have been reduced, but realistically these are meaningless without a robust mechanism for enforcing them.
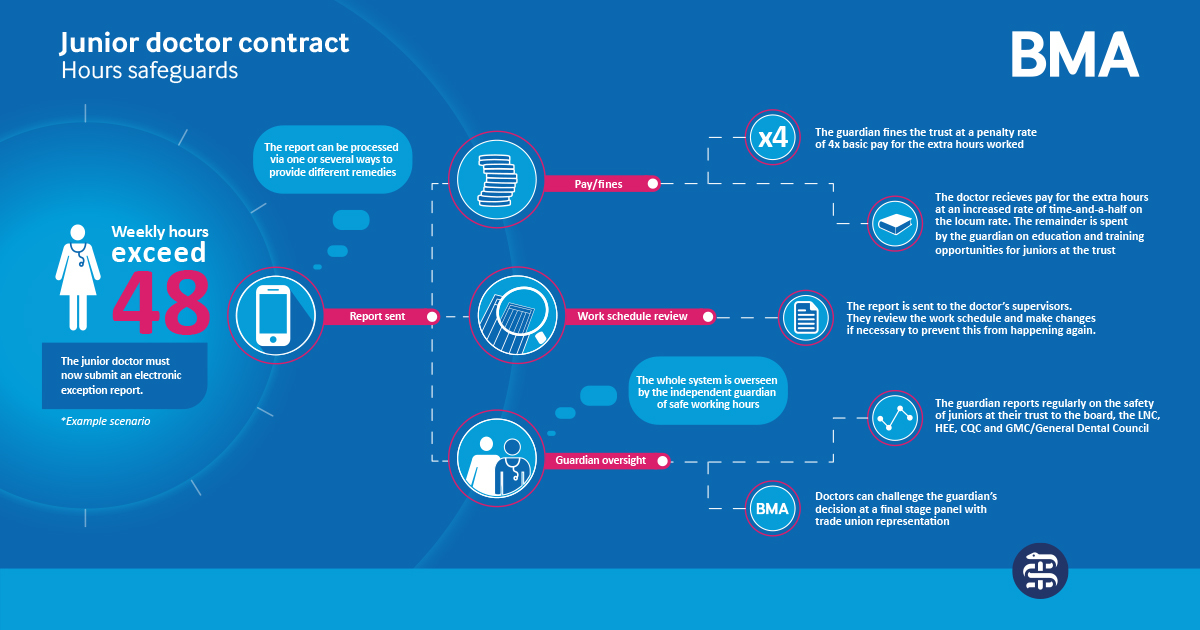
The new contract specifically removes ‘monitoring’, but more heavily involves the BMA/ local junior doctors in the process of ‘safeguarding’. This is a quick summary of the proposed new system for ‘breaches’ of hours.
- The junior doctor reports a problem – this is called an ‘exception report’. This can be a problem about overworking on hours, or the post being inadequate training.
- This ‘exception report’ goes to the junior doctors educational supervisor, with a copy to the guardian of safe working (see below) or to the director of medical education.
- An initial meeting between the junior doctor and the educational supervisor occurs where the educational supervisor reviews the report and can remunerate the doctor, make changes to their rota or do nothing.
- The junior can appeal up the chain – first to the guardian and DME and then to a panel – with the BMA or other sending a representative to sit on the panel.
- The trust will collect data on rota gaps and report this to the GMC, HEE, and GDC. A copy should go to the junior doctors forum
- The junior doctors forum will be formed by each DME and ‘advise’ the guardian on spending of funds produced from penalty fees paid to doctors who are overworked. The exact split of how much will be paid to the doctor and how much to the hospital is TBC
Here is a diagram from the BMA that outlines this process.
I have a number of issues with this system
- The process from first reporting to sitting before a panel if an exception report is not dealt with properly is approximately 16.5 weeks at a maximum. That’s through every level of escalation. Seeing as how most placements last 4 months, and the doctor isn’t going to report on day one, this seems wholly unfit for purpose
- The process puts a huge onus of responsibility on the educational supervisor, assuming powers that they certainly do not have currently, namely;
- The power to create ‘learning opportunities’ in a work schedule. Imagine an ITU consultant ‘creating’ a clinic for a trainee to sit in, or an Oncology consultant ‘creating’ a procedures list.
- The power to give time off in lieu or renumeration – mostly ES don’t work in dept or with rota managers, let alone HR – so how will this work?
- The power to remove doctors from posts and initiate system-wide changes, especially as “The educational supervisor may be in a different department, and occasionally in a different organisation, to the trainee”
- The final decision on an ‘overworked’ doctor is ‘final’ at the panel
- ‘Breaks’ – have to be taken at approx 30 minutes/5 hours or 2x 30 minutes in 9 hours. ‘Breaches’ related to missing breaks are to be ‘validated and found to be correct’ before any action will be taken. 1) Who covers during a break? Most shifts I’ve worked have been the bare minimum staff, so what is the arrangement to have a break? 2) Who is going to validate and find this correct? 3) Is it a ‘break’ when you are carrying a bleep?
- Overnight rules regarding rest are welcome – if <5 hours rest or working continuously when on-call the doctor is ‘exempt’ from the next days work. But there is no provision in the contract for anyone to cover. How do you go home as the surgical registrar for example on a saturday after on-call if there is no surgical registrar covering?
- The involvement of junior doctors in the running of their training is a good thing – but what is to stop them being sidelined in hospital? To my reading there are no mandated reporting of the guardian to the JD forum, no powers to stop a guardian appointee missing meetings and not engaging. Will this work in smaller trusts?
- The entire removal of ‘hours monitoring’ is still the worst thing about this contract. But there may be a solution – see below.
- There are many references to doctors being asked to make emergency cover arrangements, exceptional circumstances to cover rota gaps and accrual of ‘time in lieu’. Looking at the context (See linked post- Part 2) of the contract, I worry these are all clauses that will enable hospitals to stretch their workforces far farther than was previously safe. Despite the assurances that ‘breach’ penalties will be paid – the money now goes back to the hospital. This effectively removes any actual financial penalty to the hospital, and remains cheaper than hiring more substantive staff or hiring locums. In times of austerity I am concerned this will lead to hospitals relying on their juniors to plug gaps. But more on this in Part 2.
- The guardian role. I have many issues with this;
- The time commitment is ‘dependent on the size of the organisation’ but a singe guardian can still cover multiple trust sites. There needs to be a maximum number of trainees/guardian, the role has to be full time (previously advertised at 1-2 PA’s a week, equivalent to 4-8 hours work for a consultant), and must be completely independent from the board and HEE. Only independence is stipulated in the contract so far.
- ‘Funds’ distributed from ‘penalties’ can go to ‘expertise in rota design’ and ‘service improvement projects’. There is nothing stopping trusts taking ‘penalty’ money from overworking doctors and funding more HR staff, or a ‘service improvement’ project unrelated to junior doctors conditions e.g. repainting A&E.
- ‘Work schedule reviews’ are triggered when the trainee believes the rota breaches the contract hours. How a guardian, who will be a senior consultant most likely in an unrelated specialty, will change rota’d hours and work commitments in another specialty seems practically very dubious.
Overall on safety I welcome the headway that has been made on what was a travesty of a contract in March, but I still think it doesn’t go nearly far enough, facing the crisis the NHS is heading towards.
Unfair?
On equality – the contract makes some important in-roads
- The Guardian is seconded to ensure equality and diversity are respected, and that a ‘champion of flexible working’ is appointed within the educational faculty
- HEE have promised to make a review into married couples and civil partnerships, and those with caring responsibilities, to make joint applications or transfer between regions more easily. This is supposed to happen next year. We will have to watch this very closely.
- Transferring specialties for those with disabilities or care responsibilities will attract pay protection.
- The flat nodal pay structure doesn’t disadvantage women on maternity in registrar training
- Additional proposed steps for women re-entering training from maternity, or academics returning to training receiving flexible pay premia.
- Pay protection until 2022 will mean those in registrar training now will not lose out, even if they take further time out e.g. for maternity or academia
- Changing specialties may be further improved by a ‘mutual curriculum’ recognition programme to review next year
There are still issues here;
- Non-resident on-call pay allowance is proportional to the amount of time spent in work. This means that two junior doctors are paid at different rates for the same work. That is not acceptable.
- If you are non-resident but feel that going home is unsafe, the hospital will charge you for on-site accommodation, therefore you will be paying the hospital to work for them. At LTFT rates this will actually cost a significant sum per hour.
On pay
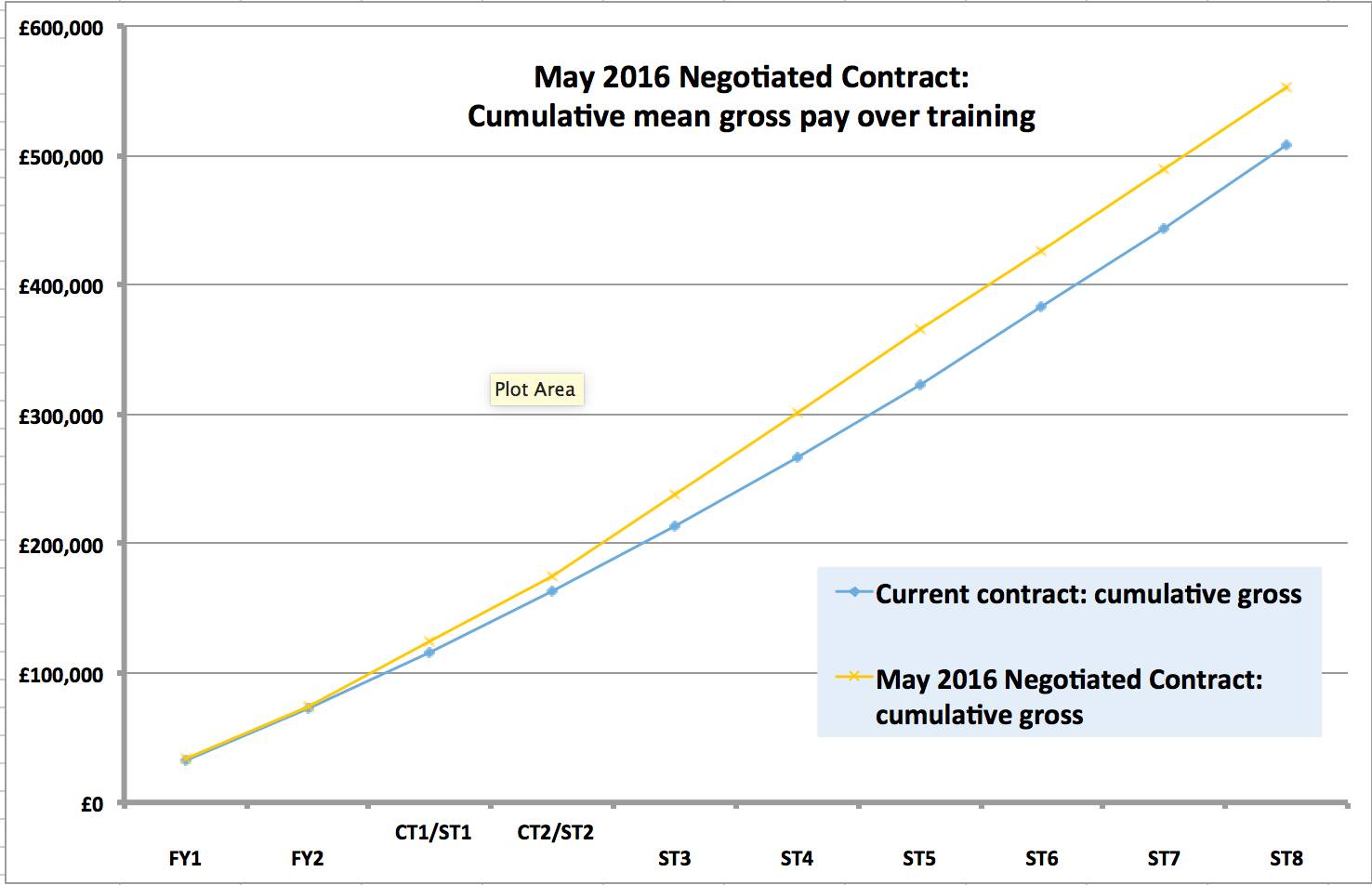
This is the most complicated part of the contract, and it’s complicated by the fact that we as a profession all work very different rotas, with different time commitments, on-call arrangements and duties, plus the point at which they are now in training. Johann has posted this cumulative comparison chart – both general and per specialties to review.
I still propose that everybody works out for themselves exactly their own earnings over their training lifetime – e.g. from F1 to ST8 or whichever, on both the old rates and the proposed contract. Remember to exclude NI (now 12%), pension pay (which is removed from your basic ONLY), and tax.
Here is a complex calculation I did – based on a medical rota of 40% 1B banding;
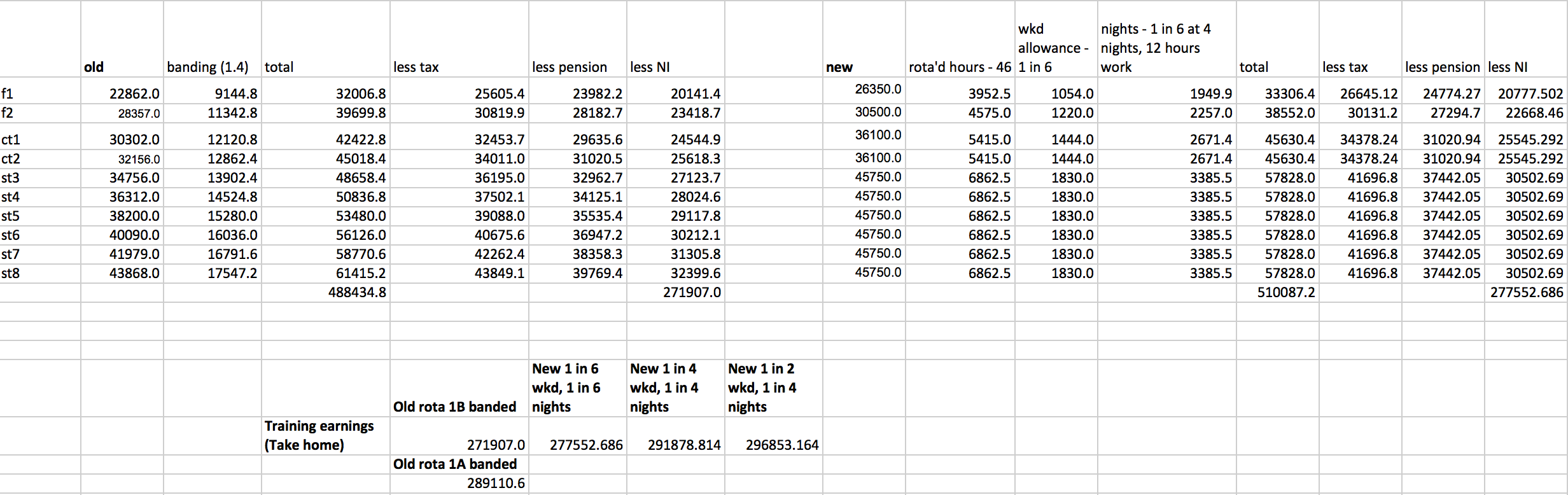
As you can see the lifetime take-home pay for a 40% 1B banding on the old rota, compared to a 1 in 6 weekends, 1 in 6 nights rota (4 nights every 6 weeks at 12/hr per night), is a very slight pay rise, over 10 years of training, of around £600/year. However on a 50% 1A banded rota, roughly 1 in 4 weekends, 1 in 4 nights rota (again 4 nights, 12hrs/shift, every 4 weeks e.g. typical ICU) it’s a slight pay increase, £300 per year take home pay. So while the ‘basic payrise’ disappears in take home pay, it does increase your pension however, I have yet to calculate exactly by how much. Whether or not this is acceptable to you is a personal opinion.
(Please post your individual calculations in the comments below with the conditions and your working, so we can get a collective sense of how everyone will be affected. Remember your vote is for yourself, but also for your colleagues.)
The real issue here is how out-of-hours work scales – the pay difference between a 1 in 4 weekends, 1 in 4 nights vs a 1 in 2 weekends, 1 in 4 nights, over your lifetime is about £500/yr. As in for working twice the weekends you were previously (and for work the definition is any hour worked on the weekend), you will be paid roughly an extra £60/month. That won’t really cover twice as much childcare for example. As pointed out previously, ‘acute’ specialties will lose out the most.
Inflation:
- It’s important to remember that with the pay freeze since 2009 Junior Doctors have lost 25% of their income.
- With further below inflation pay rises we stand to continue receiving this stealth pay cuts: 1%, 0.9% and 0.8% over the next three years, with inflation predicted to rise between 1-2.5% by 2020.
This doesn’t take into account non-resident on-call or flexible pay premia pay.
- On NROC I see two main issues.
- The ‘prospective’ average estimate is not going to actually work – shifts will vary wildly between having to be ‘at work’ and not, depending on several factors, some of them dependent on the individual doctor. The contract is very specific; ‘work’ is any clinical work, including telephone calls.
- I can imagine pressures on judgement for doctors that preferred to ‘go in’, if they are outliers in a rota where most people don’t. This creates a mechanism for monetary considerations in clinical judgement. I find this unacceptable.
- Again, the 8% on-call allowance is acceptable, as long as work done on-call is paid for at the prevailing rate, and it is still safe to regularly work the next day. This will take exceptional vigilance on behalf of individual trainees- more on that below. Again this will be overseen by educational supervisors and guardians of unsafe working.
- On flexible pay premia; for academics this is good, and for hard-to-fill specialties this may be good, although I imagine the amounts spread over training and subject to tax would make very little difference to take-home pay on a monthly basis, especially in hyper acute specialties already losing out on unsocial hours like A&E.
- Pay protection is rubbish. Please do not rely on this. The ‘cash floor’ is created by your earnings plus allowances on 31 October 2015 or 2 August 2016. This does not take into account the rise in salary you would be due if you weren’t on the new contract, and only protects your basic. Allowances for weekend and unsocial hours are calculated on your new basic, in the same way.
- Locum work: this is going to be a disaster. The assumption is the majority of us are in training and doing sneaky extortionate locum work through agencies. Forcing us to work through a staff-bank for shifts isn’t going to change a thing. Why?
- 1) Most full-time trainees cannot safely do agency locum work on top of their existing training commitments. I have probably done maybe 5 locum shifts in my career.
- 2) Most agency locum doctors are not in training- therefore unencumbered by these clauses anyway
- 3) Even if the odd shift we work on top of training was covered as an NHS bank instead of as agency bank, it would still leave the majority unfilled. Usually this worsens cover for substantive trainees, making conditions harder and dangerous.
- 4) It’s also unnecessarily punitive, and generally annoys people to think that a contract can monopolise their personal time as well as the time they spend at work.
- 5) I suspect this will actually diminish the part-time locum market, making posts harder to fill.
- Again this comes down to the context of the NHS right now – see Part 2 of this linked post.
- Pay for work done. Through the guardian system you will need to be ‘authorised’ for additional hours, either before, during or sometimes after the hours worked, if you want to be paid for them. This does not reflect our usual working practices, and the contracts refers us to our ‘manager’. I have never really known who my ‘manager’ is, and as for staying late it’s always been for emergencies, when seeking authorization is not practical or safe. Again any monetary concern interfering with clinical practice is unacceptable.
- There might be ways to sort this – but it would need to have a clearly defined ‘manager’ who is reachable 24/7, and routine acceptance of ‘after-action’ authorisations for additional hours. I can already foresee this falling apart instantly.
Overall on pay I think most people will see no difference in pay, if they stay on current rotas. However, with the proposed rotas yet to be seen, you will see a substantial drop in pay for increased unsocial hours that you would’ve previously received. If your rota goes from 1 in 4, to 1 in 2 weekends, you will be paid pretty much the same. I’m happy to be corrected on this by anyone who sees flaws here – this will need to be a collaborative effort to try to ascertain the impact the contract will have.
What else?
- There is a clause in the contract saying HEE actions are subject to reporting ‘without detriment’ to the individual junior doctor. This is regards to the Chris Day case – I have spoken with Chris and he doesn’t trust a contract clause like this to actually stand up in law. It needs a law change to back it, to protect trainees like Chris.
- Leave is only allowed during ‘non-enhanced hours’ work – which now means only between 0700-2100 and no weekends. This isn’t dissimilar to current arrangements, but if rotas increase out of hours unsocial work then actually swapping to arrange leave will be difficult.
Summary
Overall I think it comes down to trust. Do you trust your hospital and your bosses to be able to implement this contract without compromising your safe working, and to listen to your concerns if it does? Do you trust your hospital and it’s managers to honour its agreement on pay for work done, and to not create rotas which are punitive and cover a lot of excess unsocial hours? Do you trust your hospital and your health secretary to listen to your concerns when the contract is reviewed in March 2018?
This is a comprehensive FAQ from the BMA : https://www.bma.org.uk/collective-voice/influence/key-negotiations/terms-and-conditions/junior-doctor-contract-negotiations/new-contract-faqs
Think on this carefully. Then think on your vote; remember the ‘referendum’ will only guide the JDC, so if it’s close it will be far more difficult than if it is clear-cut.
This won’t be a simple vote on whether you find this contract acceptable or not. Both options will require ongoing action to ensure that the terms and conditions don’t simply slide back without our input.
If you vote yes;
- We will need a system to accurately monitor hours, to ensure not only that you are paid for work as you are supposed to be, but that hospitals are running safely, and not overstretching doctors. Without formal hours monitoring we will need to provide hard evidence, that is easy to record and easy to generate, that we need more doctors.
- We will need to take an active part in our hospitals, ensuring that the LNC is a visible entity, with real power and real support. We must be prepared to escalate and see through proceedings about breaches and training
- We must ask for reassurances that educational supervisors will evolve into the super-entities that this contract requires -that they will have power to actually do what the contract suggests they can do
- We will have to be vigilant that the contract is implemented respectfully and honestly, and report incidences where it is not – to both the local LNC and the BMA and wider community.
- We must no longer isolate ourselves if we hope to survive as a profession – don’t leave that Facebook forum even if you really want to.
If you vote No;
- We must think about what comes next – what do you want to see, and how do you want it to be achieved?
- Are you prepared to re-escalate strikes? To resign?
- We must recognise that a close vote will mean the government will accept the contract on behalf of the minority ‘Yes’. They want this to go away, and don’t wish to concede any further.
- We must recognise the ‘context’ of this contract. Will a No vote lead to benefits in the long-term? What would the junior doctor workforce look like in the future?
Now read Part 2 – the Context. Before you decide.
juniordoctorblog.com

{kind=link}
[…] THE OFFER: Part 1- the Contract. […]
[…] THE OFFER: Part 1- the Contract. […]
Thanks for taking the time to wrote all of these blogs.
There are multiple points to address here but for the moment let’s stick to simple pay.
I work it out a bit different esp nights
For ST grades basic is £22/hr x 1.37 = £30. If doing 7 nights per 8weeks on 12hr shifts this is £15,100 yr for nights. Have I gone totally wrong somewhere?
Thanks for pointing this out- I’d factored in nights as a max 10 hours because of 21.00-0700am- I just checked the contract and now we would be paid the whole shift if it started past 8 so would be 12 Hours. I calculated as four nights every 6 weeks however
Also you are making the mistake I made initially – which is calculating additional nights as 1.37x multiplier. You are paid the supplement of 0.37 – the rest is usual basic.
Section 15 specifically says the supplement of 37% is paid on any/ all hours over the night shifts. This means 1.37 for all nights shift hours surely.
Number of night shifts will be 7 per cycle (even if split 4:3). So is frequency is 1:6 or 1:8 (like my rota) will still be 7 nights.
Yes but when you calculate the supplement its an additional 0.37, not 1.37.
I calculated the pay for our current rota and came out with the following: CT1s would get 33 pounds extra a month, CT2s would loose 98 pounds a month, CT3s would get 283 pounds extra and F2s would loose 225 pounds a month (all after taxes, NI and pensions).
Over a whole registrar career we would get 44 pounds extra a month on average.
The F2 pay cut you’ve calculated is crazy. As an incoming F1 I have pay protection for 4 years now. Apparently we are 1B banded for the F1 year. How does pay protection work for my F2 year? Is it based on what the person doing my role in Oct 2015 (for banding purposes) and Aug 2016 would have got paid?
No pay protection is personal- it doesn’t matter what the person doing your role previously had. This creates a cash floor that you won’t fall
Below – e.g if you are earning 28000 as an F1 when you are protected as an f2 you can’t earn less than 28000. That’s all that means.
As an EM trainee I think the contract actually seems pretty good. Currently my fairly shit ED SHO rota can get much shitter, the new contract is unlikely to change much in terms of the rota to make it better, but actively prevents it from getting any worse, which from seeing other hospitals ED SHO rotas is certainly possible.
I do agree that the new contract is quite unfair to the NR on call specialties, and as I am unlikely to ever work on call it is difficult for me to fully understand every detail of it, but as I see it if your predicted to work 6 hours of your 12 hour on call and you end up working 7 hours, then you get paid for the extra hour. And if that happens every time you do it then it gets changed to a predicted 7 hours.
But in the same way that this new contract is unfair to the specialties that work fewer weekends, the current contract of once you’ve worked 1 in 4 then every weekend after that is free for the NHS is hugely unfair to those of us that do the >1:2 rotas.
I have been through 3 hours monitoring exercises, and every time I have asked the BMA to look into my banding the first question is “have you done hours monitoring?”, to which my answer is always (3/3 times) “yes, but there were insufficient responses for it to be valid”, to which the response is “ah well, too bad”. At least the guardian is personalised to your rota and doesn’t require 10-100 other doctors completing a form (especially when it won’t affect them directly).
The safeguards in the new contract aren’t perfect, but are way better than the old one. And with the pay for hours worked, or phoning a manager if I stay late to get paid for this, surely this system is even slightly better than the “just carry on until you go home” system. Surely the possibility of being paid/time off for your extra hours is better than no possibility of this?
And with regards to your paragraph on “do I trust my hospital not to try and fuck me over at every turn” – yes I do, most of the time I’ve been screwed over is due to incompetence rather than malice, and while incompetence is unlikely to improve I believe that more prescriptive safeguards are better than the status quo.
This may be a really silly question, but as a medical student I don’t fully understand how the pay works at the moment. From what I can see, I don’t understand how most people will be better off/at least the same under this contract. If you’re working at the moment and get banding of 40%, how does an 11% increase in basic pay and an 7.5% uplift for working 1:4 weekends make up for the loss of banding? Where does the other 12% come from?
Thanks
Night pay essentially. There’s a good breakdown on the jD forum and a link in the article to the graph which shows the breakdown. But it works out as increase in basic (11%), additional hours (most rotas are 45-48, not 40 as basic, so you get another 11% here), nights (37% plus additional hours for night shifts- depending on your rota makes a big difference) and 7.5% for weekend working. This could be higher if nights touch on weekends. You can see the breakdown in the excel spreadsheet as well.
That makes a lot more sense, thank you for your quick reply!
Cumulative pay is a useful way of looking at pay for trainees entering the new contract from the first nodal pay point. Pay rises earlier sooner, but plateaus lower. Overall no change (or only slight change).
For those of us far along enough to be ST3+ and are going to be training for more than four more years, we are forced to stay on the old pay scales, and then transition onto the new scale. So, as a cohort, we never got the early rise, but will still endure the lower plateau at the end of training.
I realise that this “only” affects a few who go past ST7 (ICM+dual specialty, neurology+neurophysiology and probably a few obscure groups), but I think we are taking a hit to allow transition to run smoothly. Probably not enough people to swing the vote, but worth pointing out.
Absolutely, and I’m not clear how pay protection works for those in that situation up to 2022. As a dual trainee planned i the ‘senior decision maker’ business might add another layer, but this has not yet been discussed. It seems more of a ploy to answer critics that say this contract had nothing to do with 7 day services or the ‘weekend effect’ which has been rather battered.
How does this work out for psychiatry trainees, esp the on call? I find it slighly confusing as I’m a final year med student abs haven’t worked yet. Thanks
One quick comment (haven’t read all those above so sorry if this is repetition) – the panel is not the final decision on an exception report. The contract doesn’t exempt hospitals from employment law hence a tribunal is the last resort, for which BMA members would be entitled to representation.