It’s my job as a doctor to interpret trends and analyse hodgepodge information to predict an outcome. I look at the NHS and see a single direction of travel: collapse without rapid and drastic intervention.
In a series of posts we will look at exactly why and how this is happening. This is what I see- you can decide yourself what you see.
In the first post here, we looked at why the NHS budget must rise 3-4% per year just to stand still.
In this post we will see exactly how this isn’t happening and what effect it’s having.
Imagine the NHS is a person- and it is very sick.
When I first see a patient we are trained to go about their assessment systematically. We first check their airway is clear of obstruction and they can breathe.
What do health systems breathe? Money. Everything has a cost, even in a free at the point of service system like the NHS.
So let’s look at our patient’s charts- as demand has risen the NHS has suffocated without proper oxygen to feed it.
Already an alarm is flashing; hospitals went from £0.6 billion surplus in 2010, to the worst deficit in NHS history- £2.3 billion in the red.
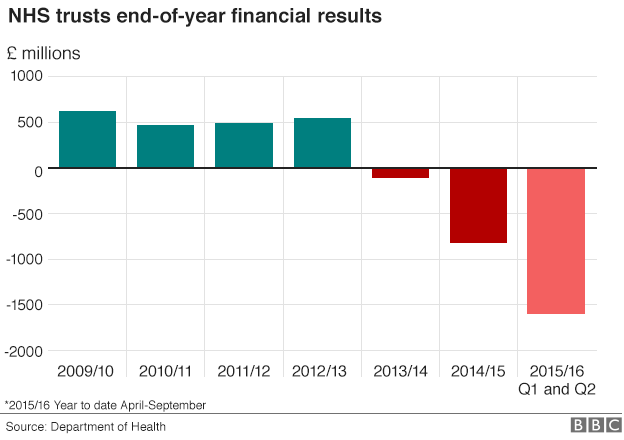
If I saw this nosedive in the hospital I would pull the emergency buzzer. We have second and third opinions here too- The Kings Fund called this
the most austere decade in NHS history.
Professor Don Berwick, patient safety tsar, said
“I know no nation that is seeking to provide [modern] healthcare at … 8% of GDP let alone 7% or 6.7%, that may be impossible “
The government spun this crisis as hospital ‘overspending‘- but that’s the equivalent of telling a gasping patient that they are ‘overbreathing’. It’s estimated the NHS needs £30 billion to keep afloat by 2020- the ‘extra’ £10 billion promised by government hasn’t appeared, is actually just £4.5 billion and is nowhere near enough. A deflated armband for a drowning man.
Next we look at the circulation, which is how the blood flows through the body and delivers life to the vital organs. What is the lifeblood of the NHS? The staff.
And we are haemorrhaging out. Just like our real blood the NHS system is made up of lots of essential components; doctors, junior and consultant and GP, nurses, midwives, paramedics, pharmacists, health visitors, radiographers, physio and occupational therapists, clerical and secretarial staff, cleaners, security. The list goes on. Every single staff group is suffering.
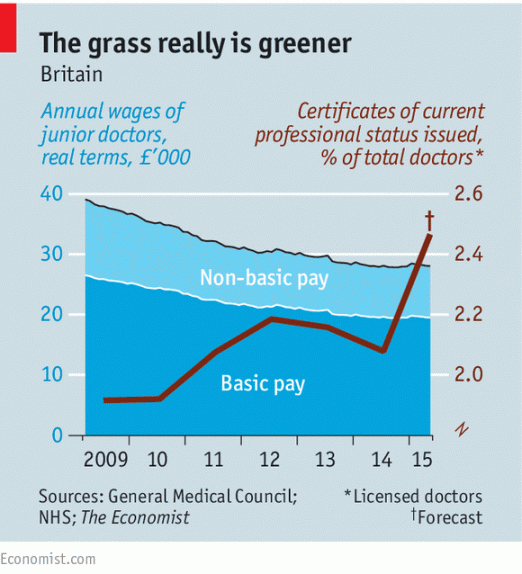
In the last two years the number of vacant posts for doctors has increased 60%, the number of gaps in nurse’s posts 50%. GPs are contemplating mass resignation, community pharmacies face mass closure, and the cuts to student nursing bursaries mean fewer nurses will be enticed into training. And junior doctors? Alongside most NHS staff junior doctors have already taken a 25% paycut in real terms since 2008, and certificates to leave the country are on the rise.
Now thanks to a toxic contract dispute they are leaving training in England; first choice applications to Scotland and Wales jumped 30-40% vs 2015, and first year training was under recruited in England for the first time in history.
The NHS needs a rapid and skilled workforce transfusion, and to stop bleeding staff burnt out by demoralising leaders and working environments.
The next step in a real patient is to assess their brain- so who are the brains? Well, Jeremy Hunt is still Secretary of State for Health, a man who looked at the above gasping and bleeding patient and declared “the NHS needs to go on a ten-year diet“. I think we need a brain transplant.
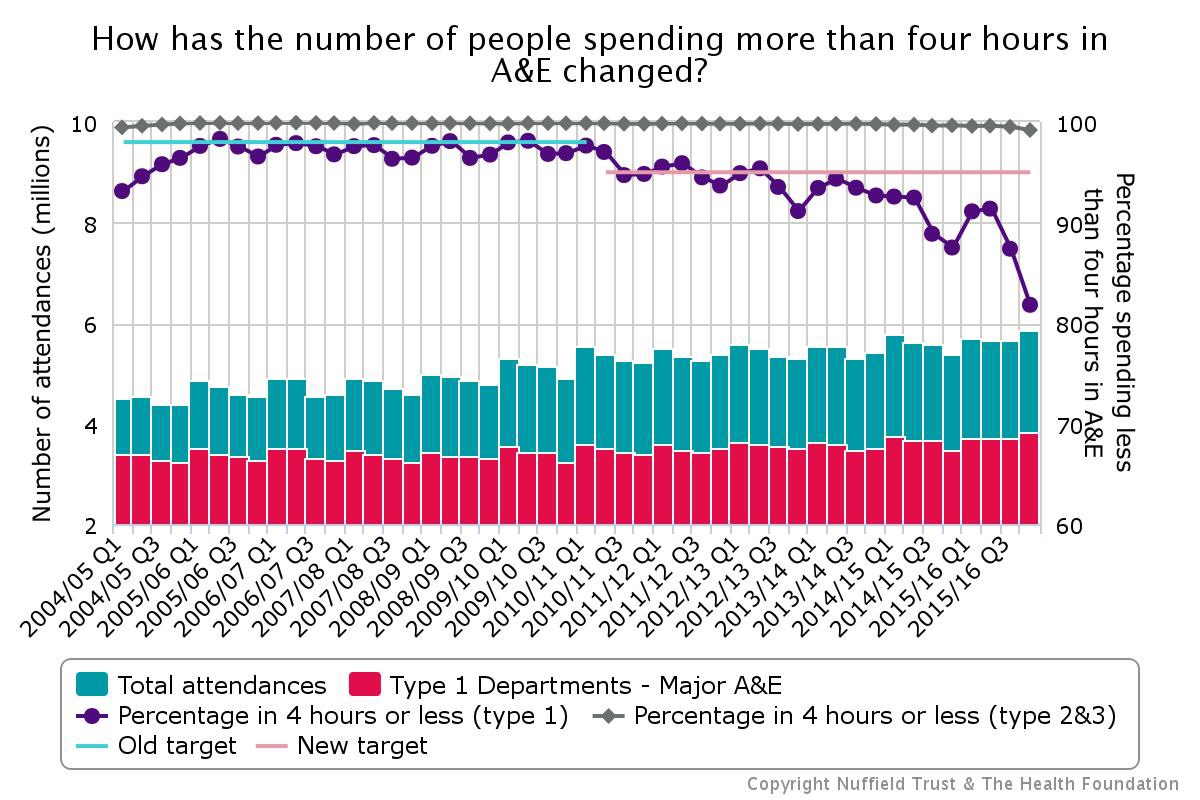
Then we assess the vital organs. What are the vital organs of the NHS? A&E, GP and cancer care. Let’s look at some test results. A&E is crashing- wait times over 4 hours just hit the highest in history, with just 81% of patients seen in target time compared to 98% just 8 years ago.
A&Es are closing and downgrading due to lack of staff and funding and no plan to cope with demand when other local departments close.
GPs are closing at record rates– and some being sold privately for more money, and for the last two years we are consistently missing cancer targets.
And let’s not forget the huge problems in social care funding. Even if we resuscitate our dying patient, we can’t forget that their house is caving in as well.
In the midst of all of this the government want to launch a ‘seven day service’, and deny there are any problems at all. Some NHS leads are even starting to leave reality altogether and claim ‘we don’t need safe staffing levels’.
Imagine a crowd of very concerned doctors and nurses around a very sick patient, tubes and wires and monitors blaring, and in jumps Mr Hunt, trying to shoo attention away and declaring “He’s just overbreathing and needs a good diet is all!”. As a doctor I would be within my rights to have him thrown out of the hospital. I can’t seem to get him thrown out of government though.
And as our leaders withhold the vital oxygen our patient NHS needs, as they fail to address the profuse haemorrhaging and the multi-organ failure, we have to ask why? Why would a responsible government be so wilfully ignorant of such catastrophe? And can we hope to resuscitate?
Find out in our final instalment;
The NHS is Collapsing Part 3: The collapse is a choice, not a necessity.
Juniordoctorblog.com
Read the other parts in this series: The NHS is Collapsing.
Part 1: A Life in a Day of the NHS
Part 2: If the NHS were a patient, I’d be pulling the emergency alarm

{kind=link}
[…] The NHS is collapsing. Part 2: if the NHS were a patient, I’d be pulling the emergency al… […]
Are you talking about the NHS in England only? That is, not NHS Wales, Scotland or Northern Ireland. I think that’s an important distinction to make but you don’t appear to have made it (in this or the previous post). Most of the figures that you’re quoting seem to relate to England only.
That is an important distinction I agree. I will clarify.
[…] The NHS is collapsing. Part 2: if the NHS were a patient, I’d be pulling the emergency al… […]