This was in the Times a few weeks ago: [1] Jeremy Hunt plans to enforce doctors work AT LEAST two years in the NHS before they can leave, to ‘payback’ the £250,000 cost of training. And then this [4] was in the Telegraph this week- MP Tom Tugendhat parroting the same, although less specific about exactly how long a doctor should be chained to the country.
Given the dark times afoot currently between the junior doctor workforce and the DoH and Mr Hunt, this feels like Mr Tugendhat is throwing his hat into the arena and the argument from above seems to ask – how much is a doctor really worth?
1) In Mr Hunt’s plan, the government will ‘force’ students to work or take away bursaries of up to £13,000. These are bursaries that pay for tuition fees and reduced rate maintenance loans, making fifth year students and above ineligible to take these on their normal student loan. This means that a student with a normal £5000 maintenance loan to pay the rent, food and transport for a full time university course will have this stopped, then reassessed by the NHS, who typically, award £2-3000 in it’s place. Many students LOSE money at this stage, and most are deemed ineligible to receive the same level of support they got the year before. Paying the rent as a full time medical student, with no summer break at all, is pretty difficult.
2) Apart from in-program year exchange schemes (only 9 in 2014) [2] within the first two years of training (the foundation programme) there is no opportunity to ‘leave’ or go into ‘private’ work. In order to gain full GMc registration and work long-term anywhere in the UK all students must finish their first year as a doctor. I’d estimate only 1-2% of doctors work abroad after the first year, but 41% of colleagues [2] did not go onto speciality training (after their second year) and many went abroad. The majority however, came back.
The ‘5000’ doctors leaving each year from Mr Tugendhat appears to be confusing the Certificate of Good Standing statistics – these are issued from the GMC at the behest of a doctor moving abroad to let the corresponding regulator know the doctor hasn’t had any fitness-to-practice problems before transferring.[13] You need this for any doctor working abroad for any amount of time- the actual number staying abroad is not known for sure, but a large proportion of this number will be 1 or 2 years ‘gap years’ in Australia or NZ, or charity work.
3) The £250,000 figure attached to medical student ‘training’ cost to the taxpayer is murkily derived, possibly from this source [3]. From what I can gather it would seem the ‘taxpayer’ cost applies only to clinical placement actually, the individual cost to the student is around £100,000, less any NHS bursary- so maybe £90,000 on average. How clinical placement cost is calculated isn’t clear- the reference is ‘personal correspondence with Health Education England’. But the figure is given as £132,698. We will come back to that shortly.
4) For junior doctors and consultants it’s even less clear.
Here is the table [3] which seems to be the media source;
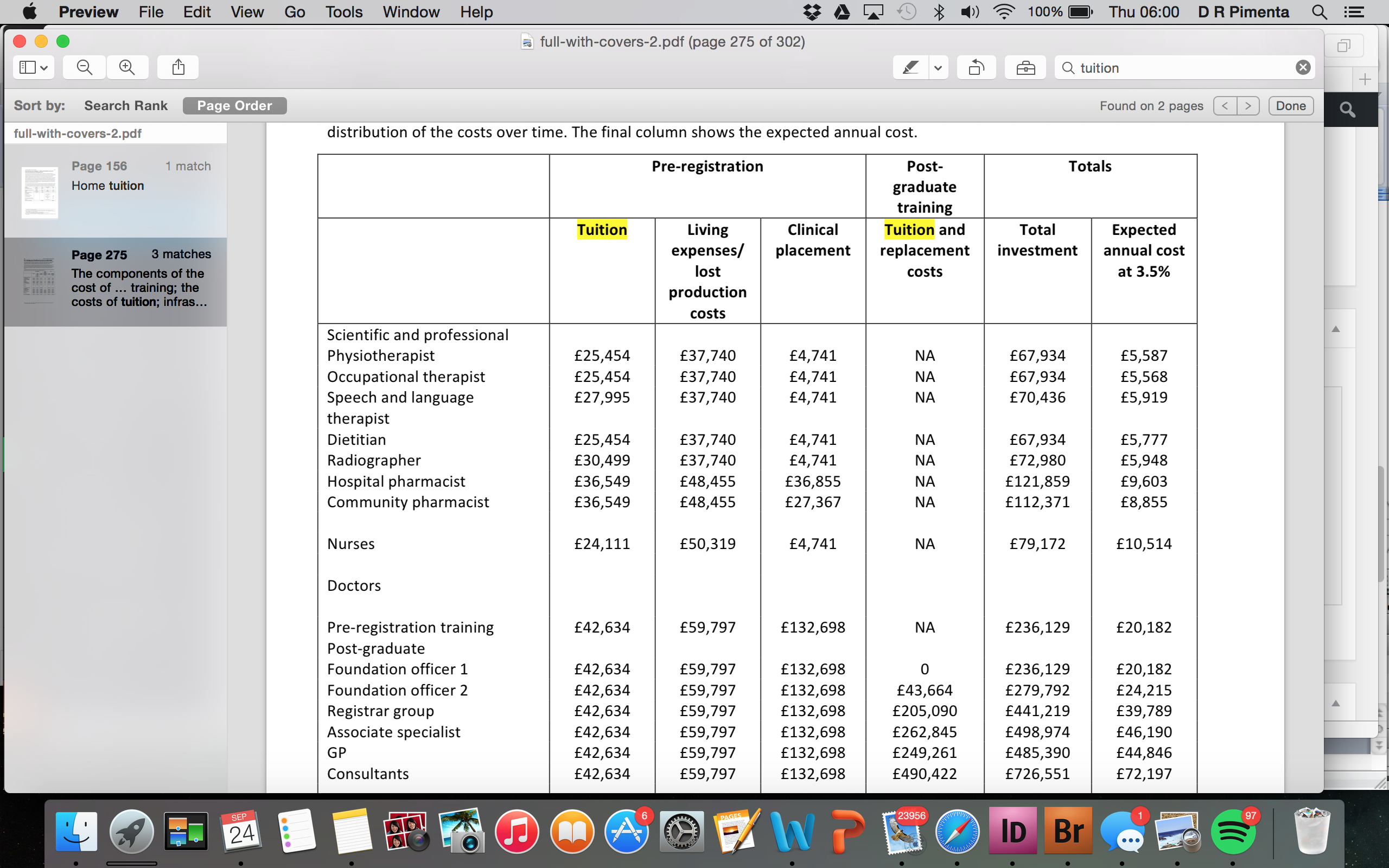
Admittedly this table is a little out of date- pre-registration ‘tuition’ should read £54,000.
The figures from Mr Tugendhat’s article come from the bottom left – GP £485,390, Consultants £726,551. How they’ve come up with these numbers appears to be to add the ‘tuition fees and living expenses’ which are paid for personally by the individual, plus clinical placements at medical school-and then added in the large column ‘tuition and replacement costs’. If you look at the breakdown of each year, starting at foundation year 1, this appears to simply be the cumulative salary over the course of training to reach GP/Consultant level, plus an additional ‘tuition cost’.
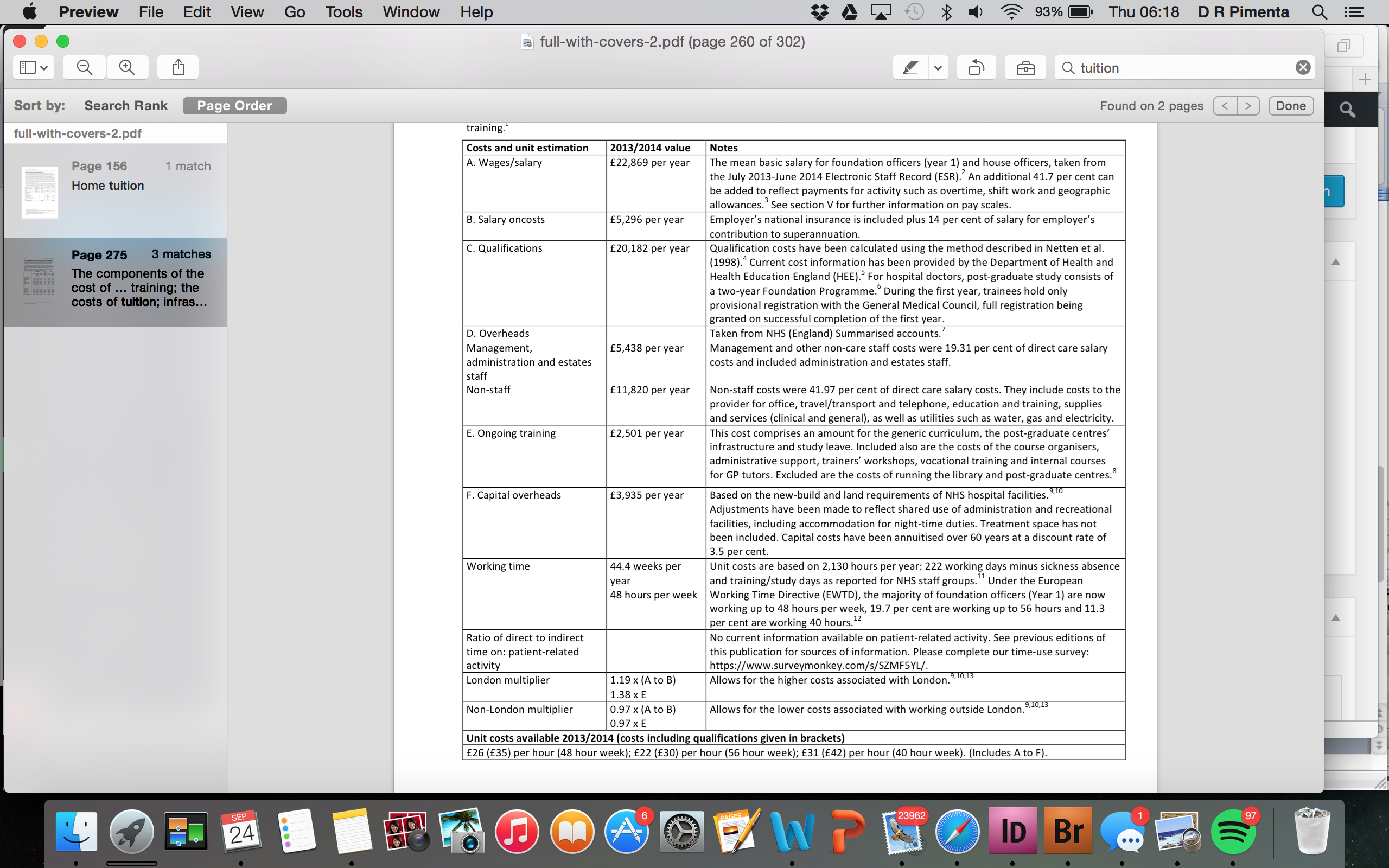
It would seem the cumulative ‘cost’ of training that everyone likes to quote actually takes into account: ‘salaried’ hours, staff costs and overheads which have nothing to do with ‘training’ – these are part of having staff to do the actual job. If you looked only at ‘ongoing training’ costs – £2501 per year for F1.
So I went ahead and re-drew the above table to try and ascertain the actual cost of ‘training’ to the taxpayer. This removes the salary as a ‘training cost’ on the assumption that 90-95% of work time of ‘junior doctors’ is spent actually working – i.e. seeing patients, writing letters, making decisions etc. It is an ‘investment’, but you can’t pay that investment anywhere else. You can’t replace the trainee doctor workforce with non-trainees at any reduced cost, so it’s inappropriate to attribute this value to ‘training’.
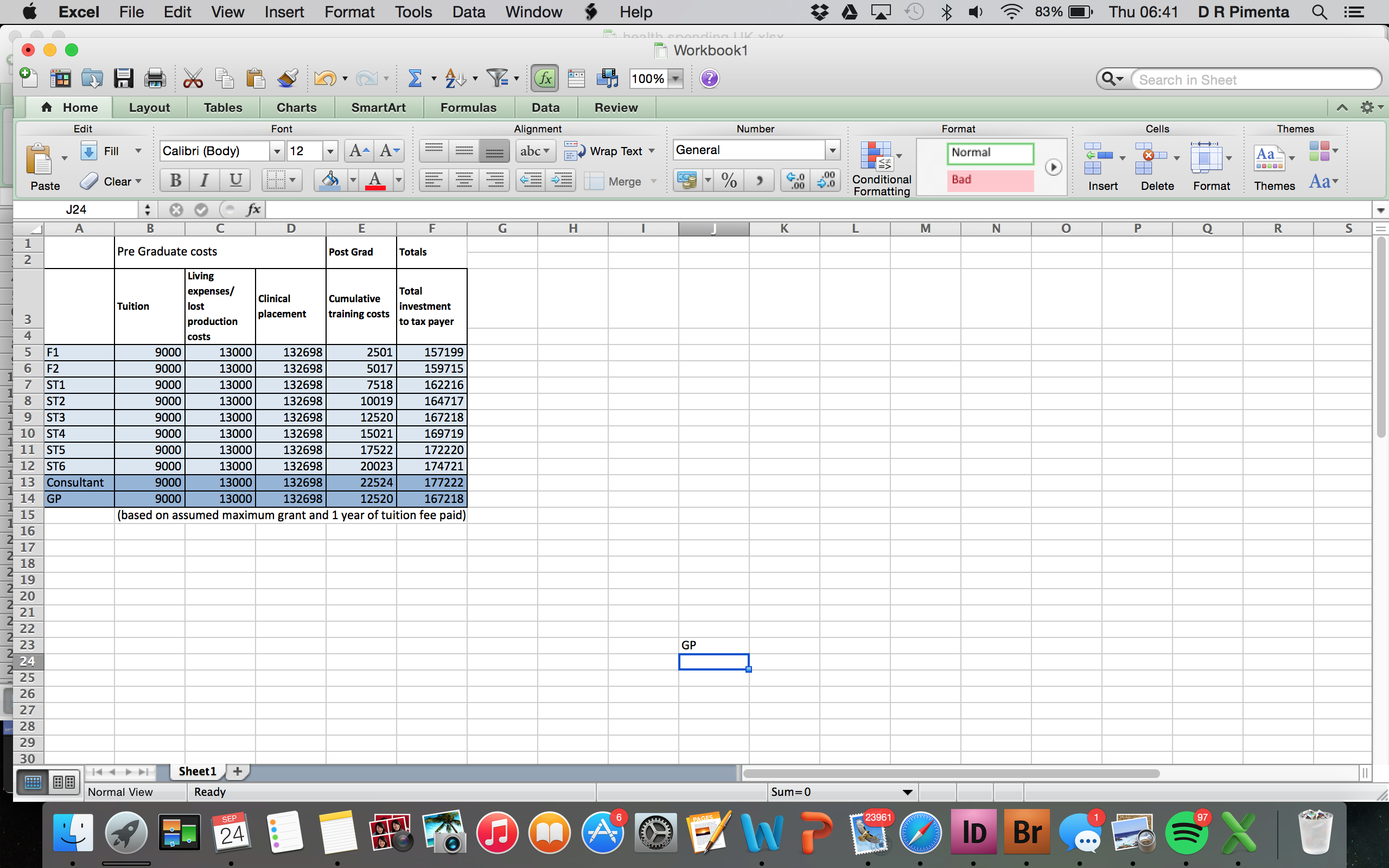
This brings the ‘taxpayer’ cost to £172,222 for a consultant and £167,218 to a GP. You will see now that most of that figure comes from the taxpayer costs for actually training medical students.
Now let’s look at the payments for medical student ‘clinical placements’ – money goes to hospitals to indemnify and host students, and money goes to some consultants and GP practices for direct teaching hours in workplaces. But who ACTUALLY teaches the students, day-to-day, for the most part of their clinical placements? Junior doctors. In fact, during my undergraduate training, except in GP, I would estimate consultant-led teaching made up only 15-30% of my total placement. The rest were foundation years, SHOs and registrars. There is no payment supplement for junior doctors- you get paid the same amount nationally whether you work in a teaching hospital or not. Every junior who teaches a student does so voluntarily and does so freely. So of that £132,000 spent on medical students, about 70% of the actual ‘training’ is done by junior doctors.
We are essentially teaching ourselves, as we have for hundreds of years.
There are actually many functions the junior doctor workforce carries out for the NHS entirely for free as well.
In my first year as a working doctor myself and several colleagues identified a serious patient safety issue with the medical handover list being passed around on bits of paper. We implemented a new electronic handover system, designed and built by another junior doctor, met with IT and medical management, trialled it’s use and then audited the patient data produced. We did this, what amounts to over 100 hours of work, entirely for free, because it benefited the patients. I don’t know what it would’ve cost to bring in an IT and management consultant to do the same project – but £50,000 isn’t an unreasonable estimate.
This isn’t an exception – this is the standard. A junior doctor is required to perform at least one Quality Improvement Project for every year of training for the NHS – this is mandatory, and free to the ‘taxpayer’. There are whole conferences filled with the benefits this has produced. [5] Many of these projects spills into genuine research, that benefits the whole field- for a junior doctor in training this is always unpaid, hours after work and at weekends and at home.
And don’t forget to mention the fact all our ‘mandatory’ training expenses, to be able to serve as the medical or surgical registrar, or to become a consultant, are paid for, 100%, by ourselves. We also pay our own license fees, or own training body subscription. This adds up – £10-15,000 over the first four years of training alone.
None of this is valued or even understood by the public at large, but worse, is not understood by the government.
We have MPs tossing these figures around comparing NHS training to military medic training, which offers three years of undergraduate paid bursaries, up to £30,000 and a lump sum of £45,000 on completion of officer training, and then a much higher basic starting salary once in post [8]*. We have MPs in a debate about junior doctor conditions being ‘surprised’ to find that [6] we do auditing work ourselves. Vince Cable is surprised at how low the basic salary for a first year doctor is.[9]
You can sit around and debate what a doctor SHOULD be paid. You could even propose an abstract formula;
(Number of doctors/number of patients) x years required for qualification x difficulty of acquisition
+ retention factor + competition from elsewhere x responsibility + life and death decision making supplement. And come out with… Splurge. Nothing really meaningful.
The real question is- how much do doctors need to be paid? As in what amount of money and working conditions keeps the workforce rested, motivated and, crucially, in the country? It is a world marketplace and contrary to popular media belief ;
1) the NHS has one of the least doctor to patient ratio in Europe [11]
1) the NHS has one of the least doctor to patient ratio in Europe [11]
2) Spends the least on healthcare in the G7 bar Italy [12]
3) pays it’s junior doctors less than Canada, US, Germany, Sweden, Scandinavia, Australia, New Zealand and many other developed countries [10]
So a pressured system, underfunded and under-doctored.
When all is said and done, it doesn’t matter what you are paying everyone else- whether a McDonalds manager earns more, or a lawyer earns less- the point is you need to pay and compensate doctors to retain them. The government have argued that the new contract would move some people’s pay up, and some down. Firstly, the proposals so far suggest that just isn’t true, and secondly I wouldn’t take a pay rise at the expense of a colleagues pay cut- we have mortgages and families to worry about. I know most of the profession would feel the same.
Lastly when we are talking about ‘junior doctors’ I am sick of listening to inane comments about new doctors trying to take blood, and only there to do ‘the paperwork’. The term applies to anyone below a consultant. We are talking about the medical registrar, the ITU registrar, the general surgical registrar- the host of brilliant men and women that turn up when the shit hits the fan at 0100am and no one knows what to do and they save your life. Or your babies life.
This isn’t just about the doctors – the government is taking increasing measures to run the NHS into the ground across the board. And once it is deplete of doctors, nurses and allied health professionals, under-resourced, and cracking all over – in will come the private hospitals, to ‘save’ the day. And many, many currently serving MPs will be rich.
So enough is enough. It’s our profession and our NHS, not theirs. We can do something. We must do something.
See you all in Australia if we don’t.
*and rightly so, given the additional training required and the inherent danger of the work.
[1] http://www.donotlink.com/ggse
[2] http://careers.bmj.com/careers/advice/view-article.html?id=20020502
[4] http://www.telegraph.co.uk/news/health/11883575/Young-doctors-must-repay-debt-to-taxpayers-before-moving-abroad.html
[5] http://internationalforum.bmj.com
[6]http://www.publications.parliament.uk/pa/cm201516/cmhansrd/cm150914/halltext/150914h0001.htm
[7] http://www.army.mod.uk/join/38414.aspx#38414
[8]https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/308383/AFPRB_DMS_Report_Final_Web.pdf
[9] http://www.bbc.co.uk/programmes/p0335sws
[10] https://fullfact.org/factchecks/are_british_doctors_among_the_best_paid_in_the_world-27442
[11] http://data.worldbank.org/indicator/SH.MED.PHYS.ZS?order=wbapi_data_value_2011+wbapi_data_value&sort=asc
[12] http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS/countries?order=wbapi_data_value_2013+wbapi_data_value+wbapi_data_value-last&sort=asc
[13] http://www.gmc-uk.org/doctors/registration_applications/img_prfr_p6.asp?p=5

In a recent Facebook discussion regarding similar issues a consultant pointed out that our “Base” salaries are paid by health education England, so therefore counts as “training”. Where’s the banding comes from hospitals and is therefore counted as service provision.
My question is, is this still the situation under the new proposals given their weighting towards Base pay over banding and extension of the sociable hours.
This would leave the hospitals with an essentially free workforce 7am-10pm 6 days a week.
This becomes more interesting and important if this agreement is still honoured if services are tendered out to private providers (as they increasingly are). Allowing them to have a largely government subsidised work force while privatising the profits.
*Insert unprofessional swear words of shock*. My nursing degree and all its associated costs were about $50,000 CAD (I lived away from home which made it more expensive). If I include bursaries, REP and Malpractice Insurance and job hunting expenses it is around ~$60,000 CAD at the highest. That was about 8 years ago. It has cost me more money to upgrade with certifications and courses (about $10,000 CAD) but if we convert CAD to GBP I am getting a great deal! We have some Brits at work who are doing their Masters here. No wonder! They told me things were rough across the pond but wow! D:
You write and research your arguments perfectly. If only a few journalists could pick up on these rational and evidence based arguments everyone would be far better informed…would you consider emailing editors of national newspapers with links to your blog for them to discover for themselves some rationality behind the soundbites? I’d suggest you also email Jeremy Hunt at Richmond House, and call his office. Also arranging an appointment with your local MP and showing him/her your research. That way, if there are any Parliamentary votes that they are involved in, they will be more well informed about the issues facing medics at the moment. I was at an event with the Home Secretary Theresa May last night, and I gave her a letter to give to Jeremy Hunt with my views. She quoted the same research about death rates at weekends, I took her to one side and quietly corrected her. Soundbites grab attention, but it would be nice for MPs to be as well informed as you are.
I agree. A very well written article that had me nodding in agreement all the way through. I’ve shared it on my FB timeline.
She must have forgotten that conversation somewhere along the line.
G’day mates. We look forward to welcoming you to Australia. We have been here a little while. Our breaking point was the great pensions robbery. I know that the Australian people thank the English for paying to train such excellent doctors ( even if this is less than they thought) and then encouraging them to come and live over here by allowing such awful pay and conditions to be imposed upon them. (The people get the government the people tolerate, we in Australia have had 5 prime ministers in as many years). The kindness of the English saves us Aussie taxpayers a bundle. It is so nice of them to give back to the colonies like this. A gift of billions of AUD over recent years already. No one knows how many doctors go to Australia and stay there? Well, yes there is. The Australian regulator aphra would have a fairly good handle on that. We look forward to seeing more of our fellow economic refugees soon. We will put the barbie on for you.
Hehe good one Jamal, but so true, people should just vote with their feet.
Great Article! i’ve been trying to debunk the 250-750K ‘cost to the taxpayer’ myth for some time and kept coming up with a blank for the costing of clinical medical school placements (50K p.a) and the annual 25K p.a. postgraduate training fees. I look forward to either catching up in either a post-renegotiated contract NHS … or out in Australia with many of our colleagues. Best wishes, GC
[…] and busiest workers” at such a late notice cancellation. Constant misrepresentation by both senior leadership in the government and the media as well as some of the most sustained tough working conditions at all levels of the […]
Hi, I’m linking some of your posts to a website (www.medicineforthenhs.com), hope that’s ok! Lucia